
- High blood sugar can overwork the kidneys, causing them to stop working properly.
- When diagnosed early, kidney disease can be slowed with treatment.
- When diagnosed later, kidney failure usually results.
- Once kidneys fail, replacement therapy via dialysis or transplant is necessary.
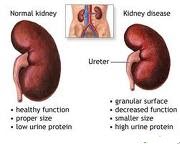
Sometimes this filtering system breaks down. Diabetes can damage the kidneys and cause them to fail. Failing kidneys lose their ability to filter out waste products, resulting in kidney disease.
How does diabetes cause kidney disease?

Diabetes can damage this system. High levels of blood sugar make the kidneys filter too much blood. All this extra work is hard on the filters. After many years, they start to leak and useful protein is lost in the urine. Having small amounts of protein in the urine is called microalbuminuria.
When kidney disease is diagnosed early, (during microalbuminuria), several treatments may keep kidney disease from getting worse. Having larger amounts of protein in the urine is called macroalbuminuria. When kidney disease is caught later (during macroalbuminuria), end-stage renal disease, or ESRD, usually follows.
In time, the stress of overwork causes the kidneys to lose their filtering ability. Waste products then start to build up in the blood. Finally, the kidneys fail. This failure, ESRD, is very serious. A person with ESRD needs to have a kidney transplant or to have the blood filtered by machine (dialysis).
Who gets kidney disease?
Not everyone with diabetes develops kidney disease. Factors that can influence kidney disease development include genetics, blood sugar control, and blood pressure.
The better a person keeps diabetes and blood pressure under control, the lower the chance of getting kidney disease.
What are the symptoms?

There are no symptoms when diabetic kidney disease first develops. Later, the following signs of decreased kidney function are:
- fatigue
- nausea and vomiting
- itchy skin
- a metal taste in the mouth
- heartburn
- swelling in the limbs and/or eyelids due to the build-up of fluid in the tissues (oedema).
What problems does diabetic kidney disease cause?

The kidneys are essential organs:
- they filter and eliminate the waste products of metabolism
- they have a central role in controlling blood pressure and fluid balance in the body
- they produce the key hormone, erythropoietin, that stimulates the bone marrow to manufacture red blood cells.
People with very poor kidney function require some form of artificial kidney support (dialysis) or a kidney transplant.
The increasing numbers of people with Type 2 diabetes has meant the demand for these facilities has been steadily climbing for several years.
Because the kidneys have a central role in controlling blood pressure, it's common for people with diabetic kidney disease to have raised blood pressure.
High blood pressure accelerates the decline in kidney function in nephropathy – in other words the two problems multiply each other’s effect. By lowering blood pressure, the rate of progression of diabetic kidney disease can be slowed down.
A target blood pressure of 130/80mmHg is recommended for diabetic patients with kidney disease.

How can you diagnose diabetic kidney disease?

The kidney filtering system normally ensures proteins are kept almost completely out of urine. In diabetic kidney disease, these filters become leaky and start to let protein through.If protein is found in your urine, diabetic kidney disease is likely to be present.
A diagnosis is made by measuring the amount of the protein albumin in the urine. The urine sample is usually taken from the first urine passed in the morning.
- A value below 20 milligrams (mg) is normal.
- A value between 20 and 200mg is called microalbuminuria (the beginning of kidney disease).
- A value above 200mg is called proteinuria (a more advanced stage of diabetic kidney disease).
If this ratio is more than 2.5mg/mmol in men or 3.5mg/mmol in women then it's regarded as significant and could require tratment with ACE inhibitors or angiotensin II antagonists.
Microalbuminuria is not a harmless stage that can be ignored until it develops into more advanced kidney disease. People with microalbuminuria are two to four times more likely to develop coronary heart disease.
Checking urine for albumin is an important part of diabetes management that should be done at least annually. Test kits are now available that allow quick checks to be done in the GP's surgery.
What are the risk factors?
There is an increased risk of diabetic kidney disease:
- with poor blood sugar control, ie levels are too high for too much of the time.
- if you smoke
- if you're male
- if there's some protein in your urine
- if you have high blood pressure
- the older your are
- the longer you've had diabetes
- if you have raised levels of cholesterol and fats (triglycerides) in the blood
- if you already have diabetic eye disease (diabetic retinopathy).
How can I prevent it?
Treatments for kidney disease
Self-care
Drugs
ACE inhibitors are recommended for most people with diabetes, high blood pressure, and kidney disease. Recent studies suggest that ACE inhibitors, which include captopril and enalapril, slow kidney disease in addition to lowering blood pressure. In fact, these drugs are helpful even in people who do not have high blood pressure.
Diet
Kidney Failure

No comments:
Post a Comment