
HEART,KIDNEYS AND URINARY TRACT INFECTION.

Heart disease is a frequent problem for people with kidney disease. Although heart disease has decreased in over the past 30 years, patients with chronic kidney disease have not enjoyed the same reduction in the chances of having a heart attack or developing heart failure. People who have diabetes, high blood pressure, high cholesterol, are overweight, smoke, have had a previous heart attack or who have close family members with heart trouble are at the greatest risk of developing heart disease.
Hardening of the arteries is the most frequent cause of heart disease. This process starts with fat deposits in the arteries and may begin at a young age, even in people without kidney disease. Over time, the fat deposits contain calcium and form plaques that can block small arteries, like those in the heart, the brain and the kidneys. Many factors contribute to hardening of the arteries. This article will consider some of the risk factors for the development of hardening of the arteries and heart disease in people with chronic kidney disease and present specific strategies for prevention.
High blood pressure is a well-known risk factor for heart disease and strokes. Blood pressure is usually reported as two numbers, the top number is the systolic blood pressure and the bottom number is the diastolic blood pressure. Both systolic and diastolic blood pressures increase the risk when they are too high, particularly in people who smoke, have diabetes or abnormal cholesterol.
A blood pressure of 130/85 is normal and it is recommended for patients younger than 65. Achieving a normal blood pressure should be the goal of therapy. For people over the age of 65, the risk of strokes is even higher than the risk of a heart attack and a blood pressure of 140/90 is suggested. Patients, who have protein in their urine or decreased kidney function, may benefit from an even lower blood pressure of 125/75, which is thought to slow down kidney damage in people who already have kidney disease.
There are several ways to lower blood pressure without taking medications. A low salt diet, quitting smoking, losing weight, exercising and decreasing the amount of alcohol you drink to no more than one glass of beer, wine, or mixed drink each day. However, most people have to take medicines to get their blood pressure low enough to decrease the risk of heart disease and protect their kidneys. On average, many people with high blood pressure will have to take three or four medications to get their blood pressure under control.
Fat in the blood stream, called lipids, contributes to hardening of the arteries. Cholesterol and triglycerides are fats in the blood stream. Both of these fats are necessary and help the body’s cells to work normally and they provide fuel for the body. Only if the levels get too high, can they contribute to hardening of the arteries. Doctors frequently measure the total cholesterol as an indication of a patient’s risk of developing heart disease. The total cholesterol consists of LDL cholesterol, the so-called bad cholesterol, and HDL, the good cholesterol. Depending on how many other risk factors for heart disease a person has, the target for total cholesterol may be as low as 200 mg/dl. The same level is desirable for triglycerides in people with several risk factors for heart disease.
Lowering the total cholesterol and particularly, the bad cholesterol decreases the risk of heart disease. People with high cholesterol levels should consider changing their diet to avoid fatty foods and other foods high in cholesterol, like red meat. However, diet alone can only lower the cholesterol by a relatively small amount and many people with high cholesterol will need to be on specific medications to lower their cholesterol levels.
Medications that lower cholesterol decrease the risk of heart disease and heart attacks. Although these medications are very effective, they may have side effects that doctors need to monitor. They can also interact with other medications that people with kidney disease may be taking. Consequently, doctors follow blood tests closely in patients taking cholesterol-lowering drugs.
Triglycerides are also a kind of fat normally found in the blood stream. When triglyceride levels are abnormally increased, they may be a risk factor for hardening of the arteries. Decreasing the amount of sugar in the diet may lower triglyceride levels and there are medications, which are also effective for that purpose.
Smoking is a very dangerous risk factor for hardening of the arteries. Smoking decreases the good cholesterol, increases blood pressure, decreases the oxygen in the blood stream and makes it easier for blood to clot in the tiny blood vessels in the heart and brain. Smoking can cause heart attacks and sudden death, particularly in patients who already have heart disease. Smoking may also worsen kidney disease. Quitting smoking is an important way to decrease the risk of strokes and heart attacks. Even among persons who have smoked heavily in the past, the risk of a heart attack can be cut in half regardless of how long or how much they have previously smoked.
Diabetes mellitus or sugar diabetes is an important cause of hardening of the arteries. Diabetes is a leading cause of blockage of the tiny blood vessels in the kidneys, heart, brain and eyes. Diabetes is also the most common cause of kidney failure. Consequently, high blood sugar levels are associated with worsening kidney function, heart attacks, strokes and blindness. Diabetes in adults is often associated with being overweight. Weight loss through sensible diet and exercise decreases the risk of heart disease and may improve diabetes control. In order to achieve the best control of blood sugar, diabetics may take medications by mouth or insulin injections. Some diabetic medicines are not good for patients with kidney disease, because they can cause acid to accumulate in the blood stream. Doctors familiar with kidney patients will avoid using these medicines.
Homocysteine is a chemical normally found in the blood that is important in making proteins. Levels sometime increase in people with chronic kidney disease and may cause hardening of the arteries. Homocysteine blood levels decrease when patients take large doses of folic acid and other B-vitamins. Doctors do not know for sure whether lowering homocysteine levels in this way decreases the risks of heart attacks and strokes.
Individuals with kidney disease are at a high risk of developing hardening of the arteries resulting in heart attacks, heart failure and strokes. Multiple factors are involved. The table below shows multiple strategies to prevent hardening of the arteries. Much of what we believe to be true about prevention is known from patients with normal kidney function. We think these strategies will work in patients with kidney disease. However, much more research is needed to learn which factors are most important and which preventive measures are most effective.
Strategies to Lower the Risk of Heart Disease
- Control Blood Pressure
- Stop Smoking
- Lower Cholesterol and Triglycerides
- Normal Blood Sugar
- Lose Weight
- Proper Diet
- Exercise
URINARY TRACT INFECTION(U.T.I)
What is the urinary tract?
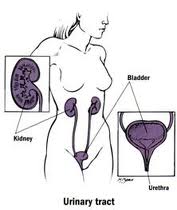
The "urinary tract" consists of the various organs of the body that produce, store, and get rid of urine. These include the kidneys, the ureters, the bladder, and the urethra.
Our kidneys are chemical filters for our blood. About one-quarter of the blood pumped by the heart goes through the kidneys. The kidneys filter this blood, and the "filtrate" is processed to separate out waste products and excess amounts of minerals, sugar, and other chemicals. Since it sees so much of the body's blood flow, the kidneys also contain pressure-sensitive tissue which helps the body control blood pressure, and some of the minerals and water are saved or discarded partly to keep your blood pressure in the proper range.
The waste products and "extras" make up the urine, which flows through "ureters" (one per kidney) into the bladder, where it is held until you are ready to get rid of it. When you urinate, muscles in the bladder wall help push urine out of the bladder, through the urethra, and out. (In men, the urethra passes through the penis; in women, the urethra opens just in front of the vagina.) When you aren't urinating (which is most of the time) a muscle called the "sphincter" squeezes the urethra shut to keep urine in; the sphincter relaxes when you urinate so that urine can flow out easily.
Urine is normally sterile -- that is, it does not normally contain bacteria. This is a good thing, since the mineral content of urine make it a great medium for bacteria to grow in. (If you have sugar in your urine, it's an even better culture medium, but that shouldn't happen unless you are diabetic, or are one of the rare people -- like me -- who are not diabetic but still have sugar in their urine.) Usually several things keep bacteria out of the urine. These include:
- The urethral sphincter: when the urethra is squeezed shut, bacteria cannot climb up the urethra from the "meatus" (the outside opening) into the bladder.
- The length of the urethra: it's a long way up to the bladder for a bacterium. (A woman's urethra is shorter than a man's, which is one reason why women are much more likely than men to get UTI's.)
- Frequent washing: any bacteria that make it into the urethra are flushed out the next time you urinate, and since most people empty their bladders almost completely when they urinate any bacteria that get to the bladder will be flushed out too. There are also valves where the ureters enter the bladder to prevent urine from "refluxing" from the bladder to the kidneys, so even if the bladder and its urine is infected the bacteria shouldn't travel up to the kidneys
How does an infection start?
The urinary tract can be infected from above (by bacteria entering the kidneys from the bloodstream and travelling downward) or from below (by bacteria entering the urethra and travelling upward).
Infection from above is most often seen in newborns with generalized infection or sepsis. If there are many bacteria in the bloodstream, some are likely to get through the filters of the kidney to the urine. This is especially likely if the filters are immature, or if there are a lot of bacteria.
In older children and adults infection most often starts from below. In small children still using diapers, stool (which is largely bacteria) can sit for some time right at the meatus; the longer it sits there, the more likely it is that bacteria may enter the urethra. Baby boys are less likely to have this happen than baby girls, because girls' urethrae are much shorter and the head of the penis isn't as likely to sit in stool. (Note, though, that bacteria can hang out in any moist, warm area, and that UTI's in boys under 1 year old seem to happens more often in uncircumcised boys than in circumcised boys since bacteria can accumulate beneath the foreskin.) Older girls may become prone to UTI's through wiping back-to-front when they are first toilet-trained, which pulls stool into the vaginal/meatal area. Sexually active teenage and adult women are more prone to UTI's because of friction at the meatus, which tends to push bacteria into the urethra (urinating after intercourse helps avoid UTI's); the same mechanism may cause UTI's in teenage boys and adult men, although they are again less prone to UTI's than women of the same age.
Where do UTI's occur in the urinary tract?
In general, the farther the organ in the urinary tract from the place where the bacteria enter, the less likely the organ is to be infected.
- Urethritis is infection/inflammation of the urethra. This can be due to other things besides the organisms usually involved in UTI's; in particular, many sexually-transmitted diseases (STD's) appear initially as urethritis. However, stool-related bacteria (the most common bacteria on the skin near the meatus) will also often cause urethritis.
- Cystitis is an infection of the bladder. (Strictly speaking, "-itis" means inflammation, and there are non-bacterial reasons for bladder inflammation, but they are much less common than bacterial infection.) This is the most common form of UTI; it can be aggravated if the bladder does not empty completely when you urinate. (Some people have valves at the bladder end of the urethra as well as at the bladder ends of the ureters. You aren't supposed to have urethral valves except for the sphincter; these "extra" valves usually prevent complete bladder emptying and make cystitis more likely.)
- Ureteritis is infection of a ureter. This can occur if the bacteria entered the urinary tract from above, or if the ureter-to-bladder valves don't work properly and allow urine to "reflux" from the bladder into the ureters.
- Pyelonephritis is an infection of the kidney itself. This can happen with infection from above, or if reflux into the ureters is so bad that infected urine refluxes all the way to the kidney.
Symptoms of UTI's

The symptoms a person has with a UTI depend on how old the person is and on where in the urinary tract the infection is located.
Urethritis usually appears as burning on urination. Often this burning occurs mainly when you start urinating, since the bacteria and infected urine in the urethra cause the inflammation but are flushed out when "fresh" urine flows through the urethra on its way out of the bladder.
Cystitis may show up as burning on urination, often in the "middle" of urination. However, it may have no symptoms other than fever, lower abdominal (way down -- just above the pubic bone) pain, or even just a funny smell or colour or appearance (cloudy, dark, even blood-tinged) to your urine.
Blood in the urine can be a sign -- sometimes the only sign at first -- of a urinary tract infection. It can result from microscopic bleeding within the kidneys, or from an abscess if the infection is far advanced. Blood can also appear in urine from a bleed anywhere between the kidneys and the urinary meatus (the end of the urethra, from where the urine emerges); in particular, cystitis can result in bleeding inside the bladder, which will certainly leave blood in the urine -- whether as blood-tinging, blood clots in the urine, or something in between. When we ask patients what part of the urine stream the blood appears in, we are trying to figure out where the blood is entering the urine: for example, blood that appears just as you start to urinate and clears up as the flow continues indicates that the bleeding is in the urethra, where it accumulates until you urinate and is then flushed out by the flowing urine. On the other hand, blood that is uniformly mixed with the urine is likely coming from the kidneys, the ureters, or the bladder.
Since your kidneys are located in your back, just below your bottom ribs, pyelonephritis may appear as pain in your back or flank(s), or in the abdomen. Fever usually (but not always) comes along with the pain. If the kidneys are severely affected, you may also start seeing some of the complications due to kidney malfunction.

Complications of UTI's
Urinary tract infections can make you pretty miserable. They can do other things, too.
The biggest problem with a UTI is if it progresses to pyelonephritis. This can result in scarring and damage to the kidney tissue. Although the kidney's filter system is pretty big, it is not infinite. If there is enough damage to the filter system, waste products can't be removed properly. This constitutes kidney failure, and if it is bad enough and long-lasting enough the only solutions are dialysis (filtering your blood through an "artificial kidney" which isn't nearly as good as the real one and requires you to sit hooked up to a lot of plumbing three times a week) or a kidney transplant (which also poses many risks and problems).
A different complication occurs if the pressure-regulation tissues in the kidney are scarred. If this is bad enough, your blood pressure may be kept too low (and you'll faint frequently at the very least) or too high (leading to strokes, heart disease, and other nasty things).
Both of these problems may occur rapidly, but only if the infection is very severe. More often, the damage done by the initial infection, even if it is not compounded by future infections, progresses over many months or years. In particular, renal failure may not be complete until long after the first UTI
How do we treat (and evaluate) a UTI?
The first step in treating a UTI is to make sure there really is one. The only certain way to know if there is a UTI is to take a sample of urine and "culture" it: try to grow bacteria from the sample. If there are bacteria, we can then test several antibiotics to see which ones kill the bacteria most efficiently.
The problem here is in getting a good sample of urine for culture. Simply urinating into a sterile cup may not stop contamination by bacteria on the skin, especially with girls. If you can control your urine, it is possible to use a "clean-catch" sample. You get this by cleaning the meatus and the surrounding area thoroughly with antiseptics (such as iodine solution), then urinating a little into the toilet before filling the sample cup, and finishing your urination in the toilet. This flushes out bacteria that may be in the urethra or meatus.
Unfortunately, small children can't cooperate well enough to do this sort of collection, even if they are toilet-trained. We can collect urine with a bag ("puck") that is taped over the meatus and genitals. However, this almost guarantees contamination by skin bacteria. We sometimes use pucks to collect samples for follow-up culture, but such samples just don't work well for the initial diagnosis where we have to know whether or not there really is an infection. For the initial diagnosis in small children we usually use a sterile catheter inserted into the bladder through the urethra (after cleaning the meatal area with iodine or another soap that kills bacteria). This may sound barbaric, but it is the only way to be sure if a small child has a UTI or not. In newborn babies who may be septic, we may go even farther and draw urine out of the bladder with a needle inserted over the pubic bone (a suprapubic bladder tap) -- which may sound even more barbaric than the catheter, but the stakes are a lot higher in a newborn baby who doesn't have the defenses against infections that older children and adults have, and a suprapubic urine culture is postive if there are any bacteria growing in it -- no ifs, ands, or buts.
Once we have diagnosed a UTI we treat the patient with antibiotics. Typical antibiotics used for UTIs include trimethoprim-sulfamethoxamole, nitrofurantoin, ciprofloxacin, levofloxacin, or their chemical relatives, and certain penicillins such as amoxicillin. In some cases, when we are pretty sure from the symptoms that you actually have a UTI, we will start antibiotics right after we get the urine culture; if the culture result shows that we need a different antibiotic, we can always change. We often repeat the culture 3-5 days after starting antibiotics to make sure that we are actually killing all the bacteria, and again soon after the antibiotics are finished to make sure we killed everything that needed killing.
We also need to make sure that the infection did not get beyond the bladder, or, if it did, that the kidneys haven't been damaged. This is usually done with "nuclear scans" in which a tiny amount of a radioactive medicine is injected into the patient's bloodstream, where it heads for the kidneys to be excreted. The medicine can be detected with radiation detecting cameras, giving a picture of the kidneys: damaged kidney tissue will appear on the picture. (Older methods involving X-rays don't produce pictures nearly as good as the nuclear scan pictures, and expose you to much more radiation. The amount of radiation involved in nuclear kidney scans is much less than even standard X-rays would give.)
Ultrasound images of the kidneys, ureter, and bladder can show abscesses that may be present, as well as abnormalities in the "plumbing" (such as duplicate ureters or blocked ureters). It won't necessarily show the source of microscopic bleeding, but if the bleeding is microscopic it may stop after the infection is treated and we may never know precisely where the blood was entering the urine.
A voiding cystourethrogram, or "VCUG", is an X-ray of the kidneys and bladder taken after a "contrast medium" (a medicine which blocks X-rays) is injected into the bladder through a catheter in the urethra. We use the VCUG to look for reflux: if there is reflux, the contrast medium will go up into the ureters, and perhaps the kidneys it the reflux is severe, and this will be visible on the X-rays. As you can imagine, this isn't very comfortable for the patient, but the VCUG is the only practical way to find out if there is reflux. If reflux is bad enough, surgery can improve valve function and reduce reflux in some patients. Milder cases of reflux will often improve as a child grows; for intermediate grades of reflux we may decide to give a child low doses of antibiotics until the reflux improves (which may take several months). The antibiotics we use to treat UTIs are excreted from the body through the kidney and urine -- in fact, that's why we use those antibiotics -- so even low doses give levels of the antibiotic in the urine that are high enough to kill the few bacteria that might stray into the bladder, and resistance isn't as much of a problem as it might otherwise be.
Please Note-Cardiac patients who are on Anti Platelet drugs like Clopidogrel should consult with their doctor if they are suffering from URINARY TRACT INFECTION ESPECIALLY HAEMATURIA(appearance of blood in the urine).

No comments:
Post a Comment